Konference: 2012 17th Congress of the European Hematology Association - účast ČR
Kategorie: Maligní lymfomy a leukémie
Téma: Non-Hodgkin Lymphoma – Biology
Číslo abstraktu: 0315
Autoři: P. Vít; doc. MUDr. Tomáš Papajík, CSc.; MUDr. Luděk Raida, Ph.D.; prof. MUDr. Karel Indrák, DrSc.; prof. MUDr. Edgar Faber, CSc.; MUDr. Ladislava Kučerová
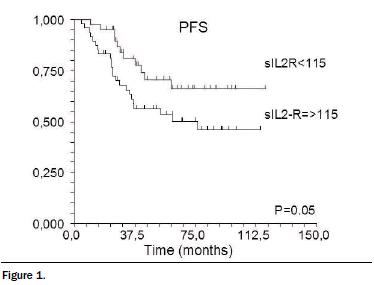
Background. Recent data show that host antitumor immunity is actively suppressed by cancer cells in many ways. The key mediator of immune tolerance is IL-2 stimulating differentiation of host CD4+ cells into suppressive CD4+CD25+ T-regulatory cells. Soluble IL-2 receptor is generated exclusively by the proteolytic cleavage of membrane IL-2R. Soluble complex IL2R-IL-2 leads to prolonged persistence of IL-2 signaling. Aims. To analyze the prognostic impact of pretreatment sIL-2R levels on FL patients’ survival in the rituximab era.Methods: We studied 88 patients with newly diagnosed FL (median age 57 years). The FLIPI risk groups were: high 43%, intermediate 27%, low 30%. Most patients (77%) had advanced-stage disease; bulk >7cm was present in 49%. Almost half of them had elevated B2M level (>3mg/L, 45%). The mean (median) sIL-2R level at diagnosis was 188.5 ±174.3 kU/L (132.6 kU/L); elevated sIL-2R ≥115 was detected in 48/88 patients (55%). The GELF criteria were met by 79 (90%) patients. Treatment was applied with respect to their disease: CHOP/CHOP-like regimen in low-intermediate-risk FL (n=40, 50%) and more intensive protocol (Promace-Cyta-BOM/adequate intensity protocol) in intermediate-risk patients with additional unfavorable risk factors (high B2M, s-TK or bulky; n=10, 13%). Nineteen (24%) patients were treated with upfront ASCT (conditioning BEAM 200) due to very high-risk disease. Rituximab was added to frontline therapy in 66% and maintenance immunotherapy with rituximab (or interferon) was applied in 31% (39%) of cases. Patients with high sIL-2R share more unfavorable prognostic features than low sIL-2R group: HFLIPI (60% vs 23%, p<0.001), bulky disease >7cm (70% vs 28%, p<0.001), advanced clinical stage (92% vs 60%, p<0.001), elevated B2M (60% vs 28%, p=0.002). No differences were observed between both groups in terms of age distribution, rituximab or maintenance application. Patients with high sIL2R needed more intensive therapy approaches: 25/29 (86%) patients treated with intensive protocol or ASCT were from high sIL2R group. By contrast, all 9 patients with no need for therapy had low sIL2R (p=0.01). Results. Complete remission rate was 83% and was comparable in both groups (81% vs 85%, p=0.67). After a median follow-up of 67 months (5.6 yrs), only 25/48 (52%) highsIL- 2R patients are alive in the 1st CR, compared to 29/40 (73%) in low sIL- 2R group. Five-year progression-free survival was 54% (95% CI 0.39-0.68) in high-sIL-2R group, compared to 66% (95%CI 0.49-0.83, p=0.05) in high-sIL 2R group. Overall survival was not significantly different between both groups (p=0.14) despite more than twice as many events observed in high-sIL-2R group (13 vs 5 deaths). Conclusions. Soluble IL-2R plays an important biological role in tumor immunosurveillance. This fact reflects the presence of advanced disease features such as bulky disease, high B2M and higher FLIPI scores. Despite application of more intensive treatment approaches, the outcome of patients with high sIL-2R is less favorable. This parameter should be considered an adverse negative prognostic factor.Supported by grants from Czech Ministry of Education (MSM 6198959205) and Faculty of Medicine and Dentistry, Palacky University Olomouc (LF-2011-006).
Haematologica, 2012; 97(s1): 126
Datum přednesení příspěvku: 14. 6. 2012


