Konference: 2015 20th Congress of the European Hematology Association - účast ČR
Kategorie: Maligní lymfomy a leukémie
Téma: ePoster
Číslo abstraktu: E1115
Autoři: MUDr. Daniela Žáčková, Ph.D.; Prof. MUDr. Zdeněk Ráčil, Ph.D.; RNDr. Eva Janoušová; Ing. Dana Dvořáková, CSc.; Mgr. Tomáš Jurček; Radek Minařík; Mgr. Jiřina Procházková, Ph.D.; RNDr. Alexandra Oltová; doc. MUDr. Barbora Weinbergerová, Ph.D.; MUDr. Lukáš Semerád; Mgr. Lenka Mokrá (Pavlovská); Prof. RNDr. Ladislav Dušek, Ph.D.; prof. MUDr. Jiří Mayer, CSc.
Background
Precise, mature data about real-world treatment efficacy in modern
era of chronic myeloid leukemia (CML) are still missing. Moreover,
true incidence of persistent side effects of tyrosine kinase
inhibitors (TKI) is rarely reported in clinical trials.
Aims
To give a real picture of TKI treatment by analyzing detailed,
prospective database of all consecutive CML cases.
Methods
Data regarding all patients treated in the academic institution
with the catchment area of about 2 million people were analyzed
according to the European LeukemiaNet recommendations (Guilhot,
Blood 2012). Diagnostic and treatment protocols follow ELN and
EUTOS recommendation/standardization. TKI side effects were
assessed according to CTCAEv4.
Results
Two hundred and fourteen patients (median age 58 years, range
18-92; 53.7% of males) with newly diagnosed CML in 2005 – 2014
underwent the analysis: 194 patients (90.7%) in chronic phase (CP),
11 (5.1%) in accelerated phase, 8 (3.7%) in blast crisis, and in 1
(0.5%) case the phase was unknown. In total, 41 (19.2%) patients
died during the follow-up (median 3.8 years, range 0.1-9.8): 22
patients due to CML activity, 13 patients due to causes probably
not related to CML, and in 6 cases the reason was unknown. The
first line therapy given to patients diagnosed in CP (Sokal high
risk in 29.9%) was as follows: imatinib, N=152 (78.4%); nilotinib,
N=24 (12.4%); dasatinib, N=6 (3.1%); other, N=7 (3.6%); none, N=5
(2.5%) due to death (N=3) and lost to follow-up (N=2) before the
treatment start. The median follow-up of 182 patients in CP treated
with 1st line TKI was 45.3 months (range, 5.2-115.8).
Estimated cumulative incidences of complete cytogenetic responses
and major molecular responses at 48 months were 92.2% and 89.2%,
respectively. Estimated OS (defined as the time from the start of
TKI therapy to the death, with no censoring at the time of therapy
change) at 48 months was 89%. Estimated PFS, FFS, EFS, and ATFS at
the same time point were 89.9%, 74.5%, 67.4%, and 66.7%,
respectively. In total, 38.5% of patients permanently discontinued
the first line TKI. The reasons for discontinuation in group
treated with imatinib (N=61/152; 40.1%) were resistance in 32/61
patients (52.4%), intolerance (13/61; 21.3%), and other reasons
(16/61; 26.2%; in 9 cases the reason was participation in
discontinuation trials, and in 5 patients non-CML related deaths).
Reasons for nilotinib discontinuation (6/24; 25%) were as follows:
resistance (N=1), intolerance (N=3), and other (N=2). Subsequent
therapy after imatinib discontinuation included dasatinib (N=19),
nilotinib (N=16), and other (N=15). After cessation of nilotinib,
patients were treated with dasatinib (N=2), imatinib (N=2), and
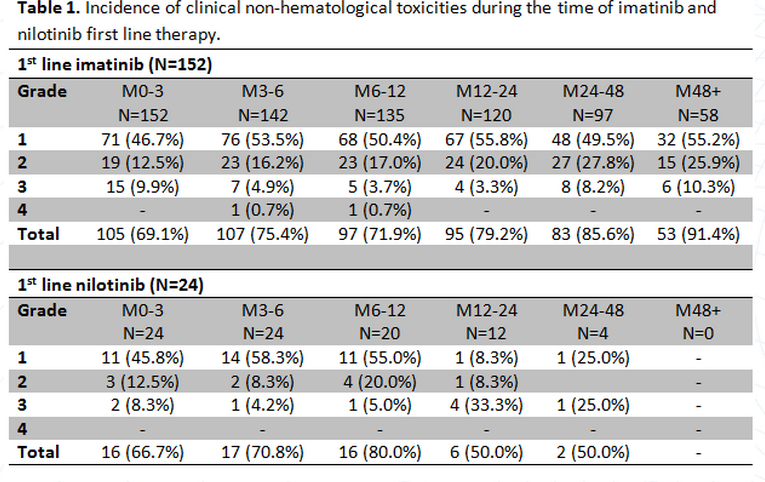
other therapy (N=2). Analysis of imatinib and nilotinib clinical
non-hematological toxicity incidence during the time revealed
significant proportion of clinically relevant events of grade 2-4,
and their persistence during the whole follow-up (Tab.
1).
Summary
About 10% of CML patients is diagnosed in advanced disease and many
newly diagnosed patients still die from leukemia. Moreover, more
than one third of patients in CP have changed the first line
therapy, mainly due to resistance, or intolerance. ATFS is a
valuable parameter covering all situations of treatment change. In
patients who continue on originally chosen TKI, there is the
evidence of clinically relevant adverse events persistence in many
of them, which can influence quality of life and can contribute to
drug non-compliance. More detailed analysis will be presented.
Keyword(s): Chronic myeloid leukemia, Imatinib,
Tyrosine kinase inhibitor
Datum přednesení příspěvku: 12. 6. 2015