Konference: 2015 57th ASH Annual Meeting - účast ČR
Kategorie: Maligní lymfomy a leukémie
Téma: 642. CLL: Therapy, excluding Transplantation: Poster II
Číslo abstraktu: 2938
Autoři: MD Paula Cramer; M.D. Asher Alban Akmal Chanan-Khan; Dr. Graeme Fraser; prof. MUDr. Fatih Demirkan; Dr. Rodrigo Santucci Silva; MD Halyna Pylypenko; M.D. Sebastian Grosicki; MD Ann Janssens; MD Andre Goy, MS; prof. MUDr. Jiří Mayer, CSc.; Marie-Sarah Dilhuydy; Dr. Javier Loscertales; Dr. Nancy L. Bartlett, MD; Dr. Abraham Avigdor; prof. Simon A. Rule; Steven Sun; Charles Phelps, MS; Michelle Mahler; Mariya Salman; Michael Schaffer, Ph.D.; Sriram Balasubramanian, Ph.D.; Angela J. Howes; Prof. MD Michael Hallek
Introduction
Recent results from the HELIOS phase 3 study in relapsed/refractory CLL/SLL demonstrated that the addition of ibrutinib to chemoimmunotherapy with bendamustine/rituximab (BR) leads to an 80% reduction in risk of progression or death compared with placebo + BR (Chanan-Khan et al. ASCO 2015). In addition to prolongation of progression-free survival (PFS; median not reached vs 13.3 months; hazard ratio: 0.203, 95% confidence interval: 0.150-0.276, p < 0.0001), overall response rate (ORR) and rates of complete response (CR) or CR with incomplete marrow recovery (CRi) were significantly improved with ibrutinib + BR (ORR: 82.7% vs 67.8%; CR/CRi: 10.4% vs 2.8%). Here we report additional analyses on the quality of response with ibrutinib combined with BR.
Methods
In total, 578 patients (pts) with relapsed/refractory CLL/SLL requiring treatment were randomized 1:1 (289 per arm) to receive BR (≤ 6 cycles) with either ibrutinib (420 mg daily) or placebo. Purine analog refractoriness (yes vs no) and number of prior therapies (1 vs > 1) were stratification factors. Pts with deletion 17p (del17p; > 20% of cells) were excluded. All pts were required to have ≥ 1 abnormal lymph node (LN; defined as a measurable lesion > 1.5 cm). The primary end point was independent review committee (IRC)-assessed PFS. In this analysis, individual parameters of response (LN, spleen, overall radiology, absolute lymphocyte count [ALC], complete blood count [CBC], and bone marrow [BM]) were evaluated. Minimal residual disease (MRD) was assessed by flow cytometry using an 8-color panel (Rawstron AC, et al. Leukemia. 2007;21:956-964); MRD samples were collected at confirmation of suspected CR (bone marrow) and every 3 months thereafter (peripheral blood). Rate of MRD-negative response was defined as the proportion of pts who reached negative disease status (< 0.01%, ie, < 1 CLL cell/10,000 leukocytes) in any sample. Reported MRD rates are based on the intent-to-treat (ITT) population.
Results
The ORR assessed by the IRC was 82.7% with ibrutinib + BR vs 67.8% with placebo + BR (p < 0.0001), and was consistent with ORR reported by the treating physician (investigator assessed) (ORR: 86.2% vs 68.9%, p < 0.0001). However, rates of CR/CRi were higher by investigator assessment (21.4%, ibrutinib + BR vs 5.9%, placebo + BR) than IRC (10.4% vs 2.8%). The IRC employed an independent evaluation of radiological scans including stringent evaluation of LN and volumetric assessment of spleen size—the main reasons for the difference in CR/CRi rates between investigator and IRC assessment.
At baseline, similar proportions of pts in each arm had bulky disease defined as LN > 5 cm (54%-58%) or abnormal spleen (~40%) as assessed by IRC. Complete resolution of previous CLL/SLL manifestations as assessed by the IRC was achieved more often in the ibrutinib + BR arm in comparison with placebo + BR for LN (34.6% vs 15.2%), spleen (56.7% vs 37.0%), overall radiology (21.1% vs 9.0%), and BM (19.7% vs 5.9%). Rates of normalization of ALC (> 90%) and CBC (> 70%) were high and similar in the 2 arms.
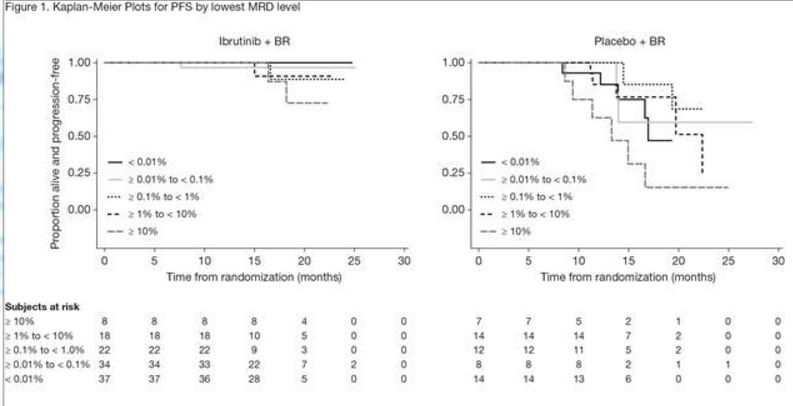
MRD was assessed in 120 pts treated with ibrutinib + BR and 57 pts treated with placebo + BR and was negative in 37 pts and 14 pts, respectively, which corresponds with an MRD-negative response rate of 12.8% vs 4.8% for ibrutinib + BR vs placebo + BR (p = 0.0011). Investigator-determined responses by different levels of MRD are shown in Table 1. The percentage of pts with an MRD level < 1% was higher with ibrutinib + BR vs placebo + BR (32.2% vs 11.8%). Moreover, the percentage of pts with an MRD level < 0.1% was higher for ibrutinib + BR vs placebo + BR (24.6% vs 7.6%) suggesting that the depth of response with ibrutinib + BR was superior. Kaplan-Meier plots by MRD level (Figure 1) show that a lower MRD level was associated with a longer PFS. However, pts in the ibrutinib + BR arm had a more sustained response at every MRD level compared with pts in the placebo + BR arm.
Conclusions
Pts treated with ibrutinib + BR showed not only a higher ORR, but also a greater depth of response, with more CRs and a higher rate of resolution of LN, spleen, and BM involvement. Furthermore, the rate and depth of MRD negativity was improved, and appeared to last longer in pts treated with ibrutinib + BR compared with pts receiving placebo + BR. With a median follow up of 17 months in the ibrutinib + BR arm, no MRD-negative pts and few MRD-positive pts had progressed, thus evaluating a trend in PFS with MRD negativity is currently limited in this arm.

Disclosures: Cramer: Gilead: Other: Travel grant , Research Funding ; Glaxo Smith Klein/Novartis: Research Funding ; Astellas: Other: Travel grant ; Mundipharma: Other: Travel grant ; Janssen: Other: Travel grant , Research Funding , Speakers Bureau ; Hoffman LaRoche: Other: Travel grant , Research Funding , Speakers Bureau . Off Label Use: Combination of bendamustine, obinutuzumab and ibrutinib for treatment of CLL. Fraser:Hoffman LaRoche: Consultancy , Honoraria ; Janssen: Honoraria , Research Funding , Speakers Bureau ; Celgene:Honoraria , Research Funding . Demirkan: Amgen: Consultancy ; Celgene: Other: Travel reimbursement . Santucci Silva: Merck: Research Funding ; Celgene: Research Funding ; GSK: Research Funding ; Janssen: Other: Travel reimbursement , Research Funding ; Hoffman LaRoche: Other: Travel reimbursement , Research Funding ;Novartis: Other: Travel reimbursement . Janssens: Mundipharma: Speakers Bureau ; Roche: Consultancy , Speakers Bureau ; Janssen: Consultancy . Goy: Allos, Biogen Idec, Celgene, Genentech, and Millennium. Gilead:Speakers Bureau ; Celgene: Consultancy , Research Funding , Speakers Bureau . Mayer: Cell Therapeutics: Other: Grants, personal fees . Dilhuydy: Roche: Honoraria , Other: Travel reimbursement ; Janssen: Honoraria , Other: Travel reimbursement ; Mundipharma: Honoraria . Bartlett: Millenium: Research Funding ; Medimmune: Research Funding ; Novartis: Research Funding ; Pfizer: Research Funding ; Genentech: Research Funding ; ImaginAB:Research Funding ; Astra Zeneca: Research Funding ; Pharmacyclics: Research Funding ; Janssen: Research Funding ; Gilead: Consultancy ; Seattle Genetics: Consultancy , Research Funding ; Celgene: Research Funding .Rule: Roche: Consultancy , Other: Travel reimbursement ; J&J: Consultancy , Other: Travel reimbursement , Research Funding ; Celgene: Consultancy , Other: Travel reimbursement ; Gilead: Research Funding . Sun:Janssen/J&J: Employment , Equity Ownership . Phelps: Janssen/J&J: Employment , Equity Ownership . Mahler:Janssen: Employment , Other: Travel reimbursement . Salman: Janssen/J&J: Employment , Equity Ownership .Schaffer: Janssen: Employment . Balasubramanian: Pharmacyclics LLC, an AbbVie Company: Equity Ownership ;Janssen: Employment , Equity Ownership . Howes: Janssen/J&J: Employment , Equity Ownership . Hallek:Boehringher Ingelheim: Honoraria , Other: Speakers Bureau and/or Advisory Boards ; Roche: Honoraria , Other: Speakers Bureau and/or Advisory Boards , Research Funding ; AbbVie: Honoraria , Other: Speakers Bureau and/or Advisory Boards , Research Funding ; Janssen: Honoraria , Other: Speakers Bureau and/or Advisory Boards , Research Funding ; Celgene: Honoraria , Other: Speakers Bureau and/or Advisory Boards , Research Funding ;Gilead: Honoraria , Other: Speakers Bureau and/or Advisory Boards , Research Funding ; GSK, Genentech:Membership on an entity’s Board of Directors or advisory committees , Research Funding ; Pharmacyclics:Honoraria , Other: Speakers Bureau and/or Advisory Boards , Research Funding ; Mundipharma: Honoraria , Other: Speakers Bureau and/or Advisory Boards , Research Funding
Datum přednesení příspěvku: 6. 12. 2015