Konference: 2012 17th Congress of the European Hematology Association - účast ČR
Kategorie: Myeloproliferativní nemoci
Téma: Plateles
Číslo abstraktu: 0611
Autoři: Prof. MD Hans Wadenvik; MD Michael Steurer; MD Ann Janssens; Dr. Philippe Quittet; Georgia Kaiafa; doc. MUDr. Tomáš Kozák, Ph.D., MBA; Prof. MD Helen A. Papadaki, PhD; MD Dominik Selleslag; Kerry Dillingham, MSc; Georg Kreuzbauer
Background. The thrombopoietin-receptor agonist romiplostim is recommended for second-line treatment of adult ITP, where the treatment goal is sustained increases in platelet counts to safe levels (Provan et al, 2010). Registrational studies of romiplostim in this setting were conducted in selected patient populations, and may not reflect routine clinical practice. Aims. Describe the use of romiplostim for the treatment of adult ITP in clinical practice. Methods. This ongoing, European, observational study enrolls ITP patients ≥18 years old, who have received romiplostim in clinical practice. Patients participating in another study, or who initiated romiplostim prior to commercial launch or have received other thrombopoietin-receptor agonists or related products are excluded. Data recorded as per clinical practice is collected for up to 2 years following romiplostim initiation, including any concomitant medications prescribed. Study outcomes include patient characteristics (at romiplostim initiation), romiplostim dose and adverse drug reactions (ADRs), summarized for patients meeting the study inclusion criteria (Full Analysis Set; FAS). We report data from an interim analysis conducted in September 2011. Results. 217 patients had enrolled, with 209 included in the FAS. Of these, 85% (178/209) remained on study, 9% (18/209) had completed the observation period and 6% (13/209) had withdrawn, with death the most common reason (11/209 [5%]). Median (Q1, Q3) age was 62.0 (47.0, 74.0) years, median weight 74.00 (64.00, 85.00) kg, and median baseline platelet count 18.0 (8.0, 33.0) x 109/L. One-third (70/209) of patients were splenectomised, 56% (116/209) female, and 76% (158/209) had received ≥3 prior ITP therapies. Median (Q1, Q3) time from ITP diagnosis was longer for splenectomised than non-splenectomised patients (9.75 [4.66, 22.18] versus 1.66 [0.22, 6.00] years). Median (Q1, Q3) duration of romiplostim exposure was 48.6 (20.1, 74.0) weeks (maximum 106 weeks), with romiplostim initiated at 1 and ≥3 μg/kg/week in 72% (150/209) and 16% (33/209) of patients. Taking the average weekly dose of all patients, the median (Q1, Q3) was 2.9 (1.5, 4.1) μg/kg/week. Platelet counts rose rapidly during the first 4 weeks of romiplostim treatment and remained >50 x 109/L thereafter (approximately 2 years). The most commonly reported ADRs were headache, thrombocytosis, arthralgia, asthenia, flushing and myalgia (2.6-7.3 events per 100 subject-years of exposure). Seven serious ADRs were reported: myelofibrosis (2 events, where the initial disease diagnosis was inconsistent with ITP and myelofibrosis more likely due to the underlying disease [MDS, metastases to bone marrow]); pulmonary embolism (2 events); drug ineffective (1 event); platelet count decreased (1 event, platelets <20 x 109/L); (reversible) thrombocytosis (1 event, platelets 477 x 109/L). No fatal ADRs were reported. Summary and Conclusions. At the time of this analysis, patients receiving romiplostim in clinical practice tended to be older and more heavily pre-treated than those enrolled in previous registrational studies. With similar doses as previously reported (Kuter et al, 2008), and no new safety signals, splenectomised and non-splenectomised patients with ITP of varying duration achieved sustained increases in platelet counts to safe levels. With the implementation of treatment guidelines, clinical practice will likely evolve to include younger, less heavily pre-treated patients.
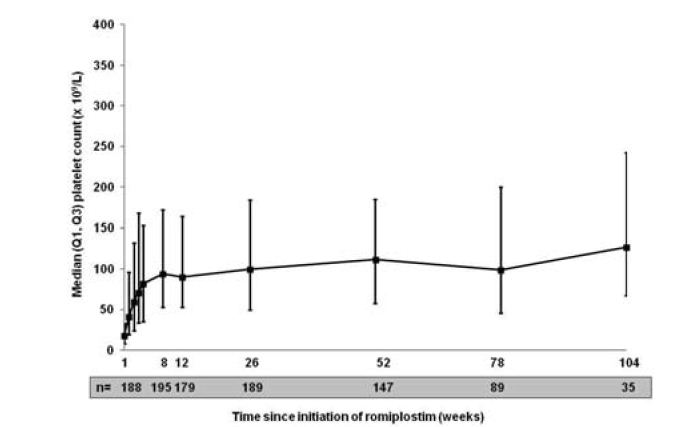
Figure 1. Platelet counts over time.
Haematologica, 2012; 97(s1): 252
Datum přednesení příspěvku: 14. 6. 2012