Konference: 2015 20th Congress of the European Hematology Association - účast ČR
Kategorie: Maligní lymfomy a leukémie
Téma: Translational studies in ALL
Číslo abstraktu: S437
Autoři: MUDr. Michaela Kotrová; Ing. Kateřina Mužíková; MUDr. Ester Mejstříková, Ph.D.; MUDr. Michaela Nováková; Mgr. Violeta Bakardjieva-Mihaylova; Mgr. Karel Fišer, Ph.D.; Mgr. Jan Stuchlý; Dr. Christianne Pott, PhD; MD Monika Brüggemann (Bruegemann), PhD; prof. MUDr. Jan Starý, DrSc.; Prof.MUDr. Jan Trka, Ph.D.; MUDr. Eva Froňková, Ph.D.
Background
Minimal residual disease (MRD) monitoring using antigen
receptor-based quantitative PCR (qPCR) became a gold standard in
the management of acute lymphoblastic leukemia (ALL), despite being
technically and financially demanding. MRD detection based on next
generation sequencing (NGS) of antigen receptor genes
rearrangements allows for a highly specific and sensitive detection
of MRD without the need for labourious optimization of
patient-specific assays.
Aims
To establish MRD detection by NGS of immunoglobulin heavy chain
(IGH) rearrangements and compare MRD levels at
BFM-protocols stratification timepoints with qPCR and flow
cytometry (FC).
Methods
The libraries for sequencing were prepared from 450ng of diagnostic
bone marrow DNA and 50ng of polyclonal DNA. Two-round PCR was used
for library preparation: in the 1st round the
IGH rearrangements were amplified with Biomed-2 FR3
primers. In the 2nd round of PCR sequencing adaptors and
barcodes were attached. Libraries were sequenced on Ion Torrent
PGM/Ion Proton sequencers.
For detection of reads containing the clonal sequence from diagnosis we used our own bioinformatics algorithm.
Results
We sequenced 213 samples from 63 patients with childhood ALL
treated according to the AIEOP-BFM-ALL 2000 protocol and 14 more
patients with relapse from previous and current frontline treatment
protocols with the median coverage 719,904 reads per sample .
Eighty-four (39.4%) samples were negative by both methods. Sixteen
(7.5%) samples were positive by NGS and negative by qPCR, and 16
(7.5%) samples were positive by qPCR and negative by NGS. This
caused a shift in risk group stratification in 30% of patients,
mainly between standard risk and intermediate risk group patients.
The overall correlation of both methods was good
(R2=0.71).
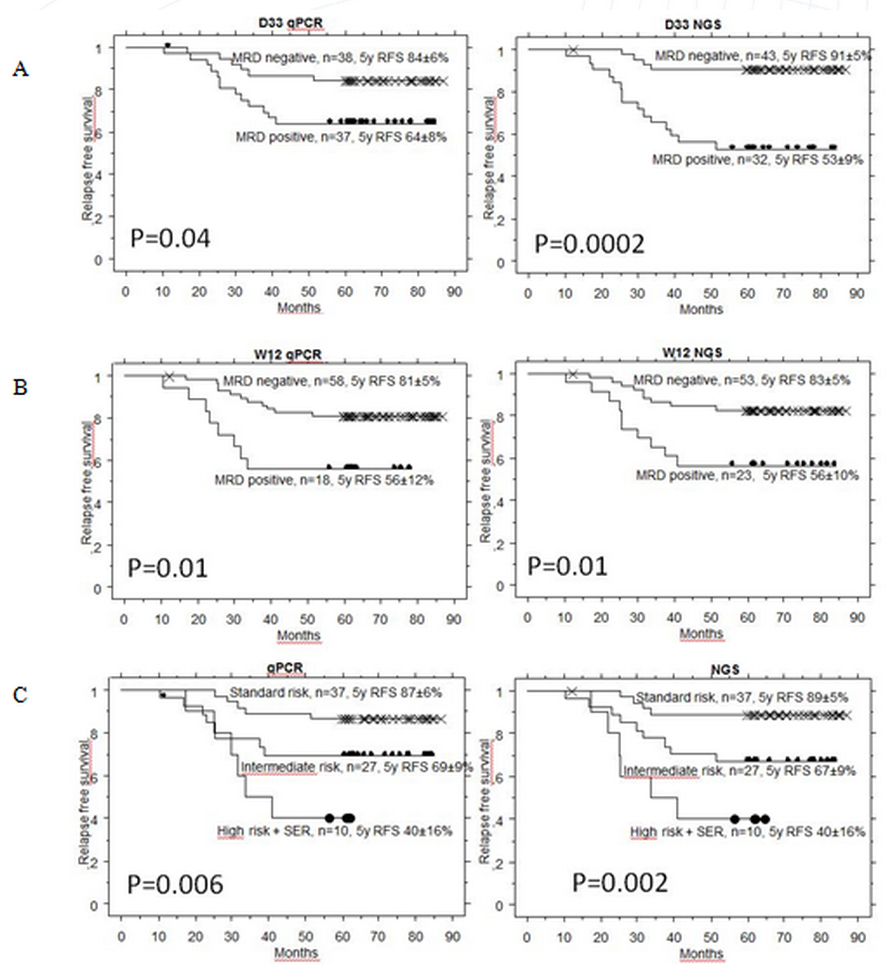
NGS approach detected significantly higher MRD than qPCR at day 33 in patients who later relapsed (p=0.001). NGS-MRD positivity at day 33 seems to provide a more accurate prediction of relapse than qPCR-MRD positivity (Fig. 1A). At day 78, the predictive value of NGS was comparable to qPCR (Fig. 1B). Combined day 33 and 78 MRD used for defining of SR, IR and HR (+SER) groups on BFM trials gave again similar results as qPCR (Fig. 1C). Similarly to FC, low NGS MRD defined a group with excellent prognosis at day 15.
Summary
NGS will speed up the process of MRD detection and provide results
at early time points, which is currently not possible due to the
long time needed for qPCR preparations. The correlation of NGS and
qPCR was good with the majority of the differrences below the
reproducible sensitivity of methods, which caused shifts mainly
between SR and IR groups.
We showed that day 33 NGS MRD
levels were higher than qPCR MRD levels in patients who
subsequently relapsed, which was reflected in a slightly better
prediction of relapse based on d33 NGS. The outcome of patients
stratified into risk groups by combined d33/d78 MRD was similar for
NGS and qPCR, despite the 30% of patients being differently
stratified by NGS.
At present, the main drawback of the Ig/TCR-exploring NGS methods
is the lack of standardization both in the experimental setting and
in data analysis. Therefore, the European network “EuroClonality
NGS Consortium”, has been formed to optimize and standardize NGS
workflow. .Before NGS based MRD can safely replace qPCR for
treatment guiding in ALL, robust results on comparability of both
methods by standardized methodology should be validated within
prospective clinical trials.
Supported by IGA NT14343, GAUK
394214 and CZ.2.16/3.1.00/24022OPPK.
Keyword(s): Acute lymphoblastic leukemia, Minimal
residual disease (MRD)
Datum přednesení příspěvku: 13. 6. 2015