Konference: 2015 57th ASH Annual Meeting - účast ČR
Kategorie: Mnohočetný myelom
Téma: 653. Myeloma: Therapy, excluding Transplantation: Poster I
Číslo abstraktu: 1844
Autoři: MD Antonio P. Palumbo; Meletios Athanasios Dimopoulos, MD; Prof. MD Philippe Moreau; Wee Joo Chng; Prof. Dr. med. Hartmut Goldschmidt; prof. MUDr. Roman Hájek, CSc.; MD Thierry Facon; Prof. MD Heinz Ludwig; prof. MUDr. Luděk Pour, Ph.D.; MD Ruben Niesvizky; M.D. Albert Oriol; MD Laura Rosiñol, PhD; M.D. Alexander Suvorov; MD Gianluca Gaidano, PhD; MUDr. Tomáš Pika; MD Katja C. Weisel; MD Vesselina Goranova-Marinova, PhD; Heidi H. Gillenwater; Nehal Mohamed; Shibao Feng; Douglas E. Joshua
Methods: Adult patients with relapsed multiple myeloma (RMM; 1–3 prior regimens) were eligible. Patients in the Kd arm received K (30-min intravenous [IV] infusion) on days (D) 1, 2, 8, 9, 15, and 16 (20 mg/m2 on D1, 2 [cycle 1]; 56 mg/m2 thereafter) and dexamethasone (20 mg) on D1, 2, 8, 9, 15, 16, 22, and 23 of 28-day cycles. The Vd arm received V (1.3 mg/m2; IV or subcutaneously) on D1, 4, 8, and 11 and dexamethasone (20 mg) on D1, 2, 4, 5, 8, 9, 11, and 12 of 21-day cycles. Treatment was administered until disease progression or unacceptable toxicity. The primary end point of the study was PFS; secondary end points included overall survival, overall response rate (ORR), duration of response (DOR), safety, and rate of peripheral neuropathy (PN). The present analyses evaluated outcomes in patients grouped according to age (ie, <65, 65–74, and ≥75 years of age).
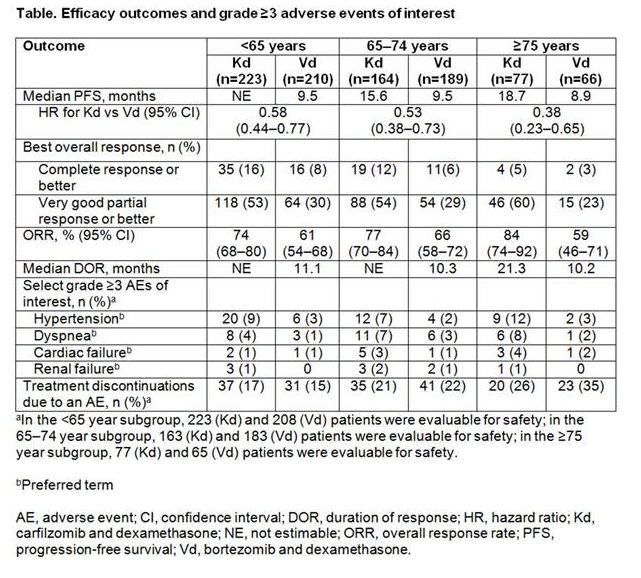
Results:A total of 929 patients were enrolled (intent-to-treat population; <65 years: Kd, n=223; Vd, n=210; 65–74 years: Kd, n=164; Vd, n=189; ≥75 years: Kd, n=77; Vd, n=66). Baseline patient and disease characteristics were generally well balanced between treatment arms within each age subgroup. PFS was improved with Kd vs Vd within each age subgroup (<65 years: median, not estimable vs 9.5 months [HR, 0.58; 95% CI, 0.44–0.77]; 65–74 years: median, 15.6 months vs 9.5 months [HR, 0.53; 95% CI, 0.38–0.73]; ≥75 years: median, 18.7 months vs 8.9 months [HR, 0.38; 95% CI, 0.23–0.65]) (Table). Kaplan–Meier PFS curves by age subgroup are shown in the Figure. ORRs in each age group were also higher in the Kd arm compared with the Vd arm in each subgroup (<65 years: 74% vs 61% [odds ratio, 1.82; 95% CI, 1.21–2.74]; 65–74 years: 77% vs 66% [odds ratio, 1.80; 95% CI, 1.12–2.89]; ≥75 years: 84% vs 59% [odds ratio, 3.75; 95% CI, 1.71–8.24]). Rates of grade ≥3 adverse events of interest, including hypertension are shown in the Table. Grade ≥3 hypertension, dyspnea, cardiac failure, renal failure were more common with Kd vs Vd within each age subgroup. Rates of grade ≥2 PN were lower in the Kd arm across all subgroups compared with the Vd arm (<65 years: 6% vs 27% [odds ratio, 0.17; 95% CI, 0.09–0.32]; 65–74 years: 8% vs 34% [odds ratio, 0.17; 95% CI, 0.09–0.32]; ≥75 years: 3% vs 43% [odds ratio, 0.035; 95% CI, 0.008–0.16]). Adverse events leading to treatment discontinuation occurred at similar frequencies in the Kd and Vd arms in the two younger-age subgroups (<65 years: 17% vs 15%; 65–74 years: 22% vs 22%), but at a higher frequency in the Vd arm for the oldest-age subgroup (≥75 years: 26% vs 35%). Deaths within 30 days post-treatment due to adverse events occurred at similar rates in the Kd and Vd arms within each age subgroup (<65 years: 3% vs 3%; 65–74 years: 5% vs 3%; ≥75 years: 4% vs 5%).
Conclusions: Kd demonstrated clinically meaningful improvement in PFS and ORR compared with Vd within all age subgroups examined, with a trend toward a greater improvement in the eldest-age subgroup (≥75 years) than in the two younger-age subgroups (<65 and 65–74 years). The eldest-age subgroup in the Kd arm had an increased incidence of select grade ≥3 adverse events of interest, including cardiac failure and hypertension, compared with the younger-age subgroups in the Kd arm. Hypertension is a recognized but manageable complication in elderly patients and should be monitored. Overall, results suggest that Kd has a favorable benefit–risk profile in patients with RMM, irrespective of age.
Disclosures: Palumbo: Celgene, Millennium Pharmaceuticals, Amgen, Bristol-Myers Squibb, Genmab, Janssen-Cilag, Onyx Pharmaceuticals: Consultancy , Honoraria ; Novartis, Sanofi Aventis: Honoraria . Dimopoulos: Janssen:Honoraria ; Celgene: Honoraria ; Onyx: Honoraria ; Amgen: Honoraria ; Novartis: Honoraria ; Genesis: Honoraria ;Janssen-Cilag: Honoraria . Moreau: Novartis, Janssen, Celgene, Millennium, Onyx Pharmaceuticals: Consultancy , Honoraria . Goldschmidt: Janssen, Celgene, Novartis: Consultancy , Honoraria , Research Funding ; Onyx:Consultancy , Honoraria ; Amgen, Takeda: Consultancy ; BMS: Consultancy , Research Funding ; Chugai, Millennium: Honoraria , Research Funding . Hájek: Janssen-Cilag: Honoraria ; Celgene, Amgen: Consultancy , Honoraria . Facon: Onyx/Amgen: Membership on an entity’s Board of Directors or advisory committees . Ludwig:Janssen Cilag: Honoraria , Speakers Bureau ; Bristol Myers Squibb: Honoraria , Speakers Bureau ; Onyx: Honoraria , Speakers Bureau ; Celgene Corporation: Honoraria , Speakers Bureau ; Takeda: Research Funding . Niesvizky:Celgene, Millennium, Onyx: Consultancy , Speakers Bureau . Oriol: Celgene, Janssen, Amgen: Consultancy , Speakers Bureau . Rosiñol: Celgene, Janssen: Honoraria . Gaidano: Celgene: Research Funding ; Morphosys, Roche, Novartis, GlaxoSmith Kline, Amgen, Janssen, Karyopharm: Honoraria , Other: Advisory Boards . Weisel:Bristol Myers Squibb: Consultancy , Honoraria , Other: Travel Support ; Celgene: Consultancy , Honoraria , Other: Travel Support , Research Funding ; Amgen: Consultancy , Honoraria , Other: Travel Support ; Janssen:Consultancy , Honoraria , Other: Travel Support , Research Funding ; Onyx: Consultancy , Honoraria ; Novartis:Other: Travel Support ; Takeda: Other: Travel Support ; Noxxon: Consultancy . Gillenwater: Onyx, Amgen:Employment , Other: Stock . Mohamed: Onyx/Amgen: Employment , Other: Stock . Feng: Amgen/Onyx:Employment , Equity Ownership . Joshua: Celgene: Membership on an entity’s Board of Directors or advisory committees
Datum přednesení příspěvku: 5. 12. 2015