Konference: 2012 17th Congress of the European Hematology Association - účast ČR
Kategorie: Mnohočetný myelom
Téma: Myeloma - Clinical 2
Číslo abstraktu: 0834
Autoři: MD Antonio P. Palumbo; prof. MUDr. Roman Hájek, CSc.; MD Martin (H.) Kropff; MD Maria Teresa Petrucci; J. Catalano; MD Michel Delforge, PhD; prof. MUDr. Zdeněk Adam, CSc.; Robert (Robin) Foa (Foà); Z. Yu; Lindsey Herbein; Christian J. Jacques; Meletios Athanasios Dimopoulos, MD
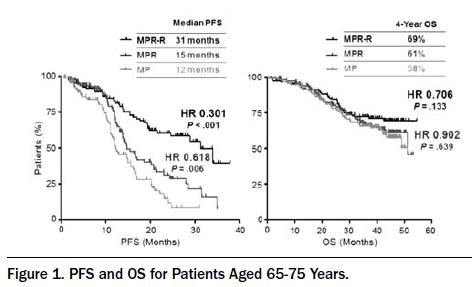
Background. MM-015 is a pivotal phase 3 randomized, double-blind, placebocontrolled trial designed to compare melphalan-prednisone-lenalidomide (MPR) induction followed by lenalidomide maintenance (MPR-R) with fixed cycle MPR and melphalan-prednisone (MP) induction in transplant-ineligible newly diagnosed multiple myeloma (NDMM) patients. Interim results demonstrated unprecedented progression-free survival (PFS) improvement (Palumbo A, et al. Blood 2011). Aims. Examine efficacy and safety in patients 65-75 years as a protocol-specified age group. Methods. Dosing and schedule have been described. Efficacy and PFS data are provided through the last adjudicated assessment (median follow-up of 27 months). The median follow-up for safety and overall survival (OS) is 41 months. Results. A total of 152, 153, and 154 patients were randomized to MPR-R, MPR, and MP, respectively. Median PFS was significantly improved with MPR-R (31 months) vs. MPR (14 months; P<.001) and MP (13 months; P<.001). A landmark analysis calculating PFS from the time of maintenance entry demonstrated that lenalidomide maintenance significantly prolonged median PFS (26 months from maintenance entry) vs. placebo (7 months) (HR=0.34; P<.001). Lenalidomide maintenance extended PFS independent of induction response (partial response vs. very good partial response or better), ISS stage (I/II vs. III) and age (65-75 years vs. >75 years). Patients aged 65-75 years were evenly distributed: 76% MPR-R patients (116/152), 76% MPR (116/153), and 75% MP (116/154). In these, MPR-R significantly prolonged median PFS vs. MPR and MP (Figure). Importantly, MPR induction alone improved PFS vs. MP (Figure). Lenalidomide maintenance reduced the progression rate by 65% (P<.001). PFS improvements were noted in all patient subgroups (renal function, induction response, and ISS stage), and an OS trend has been observed (Figure). MPR induction had a manageable safety profile, allowing 67% of patients to reach maintenance. The most frequent adverse events (AEs) were hematologic. For patients aged 65-75 years, grade 4 neutropenia occurred in 31% (MPR) and 7% (MP); grade 4 thrombocytopenia was reported in 11% (MPR) and 4% (MP). Grade 4 febrile neutropenia was not reported. The most common grade 3/4 non-hematologic AE was infection (8% vs. 6%). Discontinuation from MPR and MP induction for AEs occurred in 12% and 4%, respectively. During lenalidomide maintenance, the most common AEs were grade 3/4 infections and bone pain (5% each). Eight percent discontinued lenalidomide maintenance due to AEs. Secondary primary malignancy (SPM) were uncommon corresponding to low incidence rates per 100 patient-years of 3.04, 2.57, and 0.98, respectively, which represent a total of 12 (MPR-R), 10 (MPR), and 4 (MP) SPM. Similarly, the risk of progression/death was higher than the SPM risk. Conclusions. Continuous lenalidomide treatment with MPR-R significantly extended PFS vs. MP and MPR. MPR induction significantly extended PFS vs. MP in patients aged 65- 75 years. The manageable safety profile of MPR induction allowed 67% of patients to reach maintenance. Lenalidomide maintenance extended PFS in all patient subgroups analyzed. SPM were uncommon, although imbalanced across treatments. Overall, the risk of progression/death clearly outweighs the SPM risk. MPR-R should be considered a standard of care in transplant-ineligible NDMM patients aged 65-75 years.
Haematologica, 2012; 97(s1): 341
Datum přednesení příspěvku: 14. 6. 2012