Konference: 2012 17th Congress of the European Hematology Association - účast ČR
Kategorie: Mnohočetný myelom
Téma: Myeloma - Clinical 2
Číslo abstraktu: 0833
Autoři: M.D. Shaji Kumar; Prof. MD Philippe Moreau; Evangelos Terpos; prof. MUDr. Roman Hájek, CSc.; Prof. M.D. Gareth J. Morgan, FRCP, FRCPath, Ph.D.; Jae Hoon Lee; Stefan Knop; Wee Joo Chng; MD Paul Gerard Guy Richardson; MD Pieter Sonneveld, PhD.; Prof. M.D. Jesús San Miguel, Ph.D.; Vânia Tietsche de Moraes Hungria; Angelo Maiolino; Antje Hoering; Wenming Chen; J. Hou; prof. MD Meral Beksac; Juan José Lahuerta; MD Xavier Leleu, PhD; Prof. Dr. Joan Bladé, PhD; Brian G.M. Durie
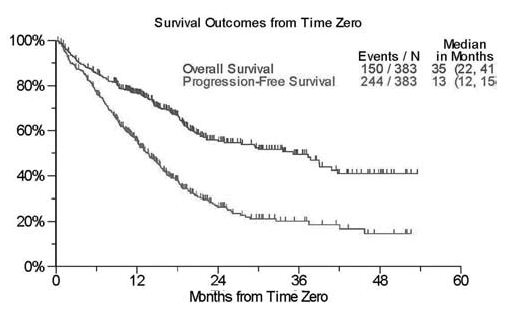
Background. Multiple myeloma remains incurable with current approaches and the disease invariably relapses after responding to initial therapy. There is no uniform approach to the management of relapsed disease and is dictated by the response to initial therapy, types of initial therapy and availability of new drugs. The outcomes associated with current approaches in this group of patients have not been systematically examined. Patients and Methods. We enrolled 383 patients with myeloma who had the first relapse of their disease between Jan 1, 2007 and June 30, 2010. Of the 383 patients, 26 were from North America, 220 were from Europe, 106 were from Asia, and 31 were from South America. Clinical data was collected using detailed case report forms for uniformity. Time Zero (T0)was defined as the date of the first anti-myeloma treatment after first relapse. The Institutional Review Board at the respective institutions approved the study. Results. Across the study, 61% were male and 49% were over 65 years at T0. ISS stage distribution at diagnosis included 26, 40 and 33% of patients in stages 1, 2 and 3, respectively. A variety of regimens were used at first relapse; bortezomib containing regimens were used most commonly (54%), followed by lenalidomide (25%) and cyclophosphamide (21%) containing regimens. The overall response rate (>=PR) to the first regimen after relapse was 58% including 14% with a complete response. The response rates were higher for the US and European centers (62 and 64% respectively). In a multivariate analysis, ISS stage 3, ISS stage 3 at relapse and Asian center were predictive of a lower response rate. There was a progressive decrease in the response rates with successive regimens; 45%, 30% and 15% for regimens 2, 3 and 4 respectively. Of the 109 patients considered eligible for stem cell transplant, 39% received an SCT as salvage therapy. Lenalidomide use was considerably lower in the Asian cohort, while bortezomib use was comparable across the regions. The median progression free survival (PFS) from T0 was 13 mos and overall survival (OS) was 35 mos, for the entire cohort. In a univariate analysis, ISS stage 3, presence of cytogenetic abnormalities, history of plasma cell leukemia or extramedullary disease, bone marrow PC% > 33% and presence of renal insufficiency were all associated with a shorter PFS as well as shorter OS (P<=0.01). In a multivariate analysis including the maximum number of variables, ISS stage 3 and presence of EMD were most associated with short OS. Conclusions: Median progression free survival for current second line regimens, which typically contain bortezomib or lenalidomide in combinations appear to be around 1 year with an OS from first relapse of about 3 years. The OS from first relapse is nearly double that seen in a cohort of patients in first relapse prior to introduction of new drugs. Clear-cut regional differences can be seen in terms of patterns of drug use and health care resource utilization and likely reflect drug availability and healthcare costs.
Haematologica, 2012; 97(s1): 341
Datum přednesení příspěvku: 14. 6. 2012