Konference: 2015 20th Congress of the European Hematology Association - účast ČR
Kategorie: Mnohočetný myelom
Téma: Late Breaking Abstracts 2
Číslo abstraktu: LB2071
Autoři: Meletios Athanasios Dimopoulos, MD; Prof. MD Philippe Moreau; MD Antonio P. Palumbo; Douglas E. Joshua; prof. MUDr. Luděk Pour, Ph.D.; prof. MUDr. Roman Hájek, CSc.; MD Thierry Facon; Prof. MD Heinz Ludwig; M.D. Albert Oriol; Prof. Dr. med. Hartmut Goldschmidt; MD Laura Rosiñol, PhD; MUDr. Jan Straub; M.D. Alexander Suvorov; MD Carla Araujo; Elena Rimashevskaya; MUDr. Tomáš Pika; MD Gianluca Gaidano, PhD; MD Katja C. Weisel; MD Vesselina Goranova-Marinova, PhD; prof. MUDr. Anthony Schwarer; Dr. Leonard Minuk; MD Tamas Masszi, PhD; Ievgenii Karamanesht; M.D. Massimo Offidani; Vânia Tietsche de Moraes Hungria; MD Andrew Spencer; Heidi H. Gillenwater; Nehal Mohamed; Shibao Feng; Wee Joo Chng
Background
Bortezomib and dexamethasone (Vd) is a standard-of-care regimen for
RMM. Carfilzomib (20/27 mg/m2; 2–10 min intravenous
[IV] infusion) is approved in Argentina, Israel, Mexico, and the
United States for relapsed and refractory multiple myeloma and
significantly improved progression-free survival (PFS) when given
with lenalidomide and dexamethasone for RMM in the phase 3
study ASPIRE (NCT01080391; Stewart et al, N Engl J Med,
2015). In study PX-171-007 (NCT00531284), carfilzomib
(20/56 mg/m2; 30-minute infusion) and dexamethasone
(Kd) had promising activity in pts with RMM (Papadopoulos et al,
J Clin Oncol, 2015).
Aims
ENDEAVOR (NCT01568866) compares Kd with Vd in pts with RMM. Results
from a prespecified interim analysis are presented.
Methods
Adults with RMM (1─3 prior treatments) were eligible. Pts were
randomized 1:1 and stratified by prior K or V (yes vs no), prior
lines of treatment (1 vs 2–3), International Staging
System stage (1 vs 2–3), and intended route of V (IV vs
subcutaneous [SC]). The Kd arm received K (30-min IV infusion) on
days (D) 1, 2, 8, 9, 15, 16 (20 mg/m2 on D1, 2 [cycle
1]; 56 mg/m2 thereafter) and dexamethasone (20 mg) on
D1, 2, 8, 9, 15, 16, 22, 23 of a 28-day cycle. The Vd arm received
V (1.3 mg/m2; IV or SC) on D1, 4, 8, 11 and
dexamethasone (20 mg) on D1, 2, 4, 5, 8, 9, 11, 12 of a 21-day
cycle. Cycles were repeated until disease progression or
unacceptable toxicity. The primary end point was PFS assessed by an
independent review committee. Secondary end points include overall
survival (OS), overall response rate (ORR), duration of response
(DOR), rate of peripheral neuropathy (PN), and safety.
Results
In total, 929 pts (Kd: 464; Vd: 465) were randomized. In the Vd
arm, 83.6% of pts received SC bortezomib. Median treatment exposure
was 39.9 weeks (Kd) and 26.8 weeks (Vd). Kd led to a 47% decrease
in the risk of progression or death (hazard ratio, 0.53; 95%
confidence interval [CI], 0.44–0.65; P<.0001), with a
median PFS of 18.7 months (95% CI, 15.6–not estimable) in the Kd
arm vs 9.4 months (95% CI, 8.4–10.4) in the Vd arm. OS data were
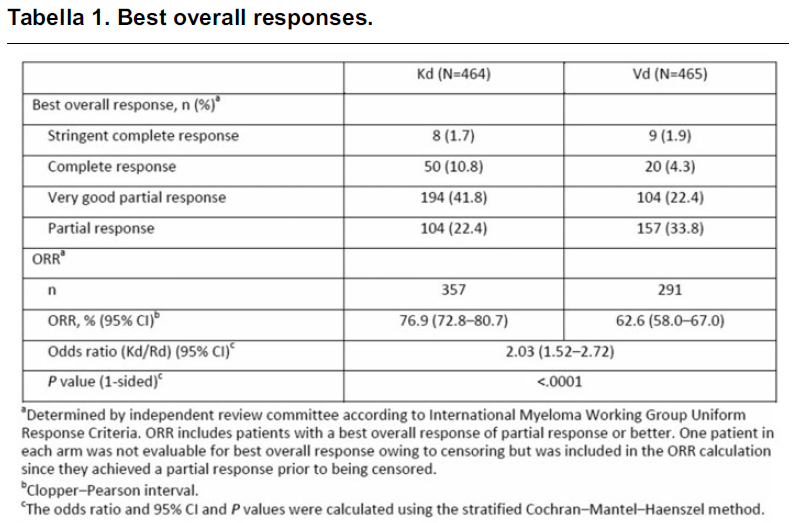
immature (deaths: Kd=75; Vd=88); pts continue to be followed. Best
overall responses are presented in the table. The median DOR was
21.3 months (Kd) and 10.4 months (Vd). Treatment
discontinuation due to an adverse event (AE) occurred in 14.0% (Kd)
and 15.7% (Vd) of pts. An AE led to dose reductions of K or V in
22.9% and 47.8% of pts, respectively; 61.9% of dose reductions in
the Vd arm were due to neuropathy-related AEs vs 6.6% in the Kd
arm. Rates of grade ≥2 PN (grouped term) were 6.0% in the Kd arm vs
32.0% in the Vd arm (P<.0001). The most common
hematologic AEs (preferred terms; all grades) in the Kd and Vd
arms, respectively, included anemia (39.3% vs 27.0%) and
thrombocytopenia (20.5% vs 17.1%); the most common nonhematologic
AEs (preferred terms; all grades) included diarrhea (30.9% vs
38.4%), fatigue (29.4% vs 28.5%), and dyspnea (28.5% vs 13.2%).
Grade ≥3 AEs of interest in the Kd and Vd arms, respectively,
included hypertension (preferred term; 8.9% vs 2.6%), dyspnea
(preferred term; 5.4% vs 2.2%), cardiac failure (grouped term; 4.8%
vs 1.8%), and acute renal failure (grouped term; 4.1% vs 2.6%). A
total of 3.9% of pts in the Kd arm and 3.4% of pts in the Vd arm
died on study owing to AEs.
Summary
Carfilzomib and dexamethasone demonstrated statistically
significant and clinically meaningful superiority over bortezomib
and dexamethasone in RMM, with a 2-fold improvement in median PFS
and a favorable benefit–risk profile. These data suggest that
carfilzomib could be a best-in-class agent for RMM.
Datum přednesení příspěvku: 14. 6. 2015