Konference: 2012 17th Congress of the European Hematology Association - účast ČR
Kategorie: Mnohočetný myelom
Téma: Myeloma - Clinical 1
Číslo abstraktu: 0298
Autoři: MD Michel Delforge, PhD; Meletios Athanasios Dimopoulos, MD; prof. MUDr. Zdeněk Adam, CSc.; prof. MUDr. Roman Hájek, CSc.; Z. Yu; Lindsey Herbein; Christian J. Jacques; MD Antonio P. Palumbo
Background. Lenalidomide is an IMiDR immunomodulatory agent with a dual mechanism of action comprised of tumoricidal and immunomodulatory effects. MM-015 is a pivotal, phase 3, randomized, double-blind, placebo-controlled trial comparing MPR-R with MP and MPR in transplant-ineligible NDMM patients. Interim results demonstrated significant median progression-free survival (PFS) improvements with MPR-R (31 months) vs. MP (13 months; P<.001) or MPR (14 months; P<.001). Aims. This analysis focused on the MM-015 safety profile and adverse event (AE) management; median follow-up was 41 months. Methods. Treatment details have been presented (Palumbo A, et al. Blood. 2011). AEs were graded according to the National Cancer Institute Common Terminology Criteria for AEs (V.3.0). For grade 4 hematologic and ≥ grade 3 non-hematologic AEs, treatment was withheld for the remainder of the cycle and restarted at a lower dose in subsequent cycles. Granulocyte colony-stimulating factor (G-CSF) or erythroid-stimulating agents were encouraged for grade 4 neutropenia or anemia. All patients received low-dose aspirin or other thromboprophylaxis where aspirin was contraindicated.
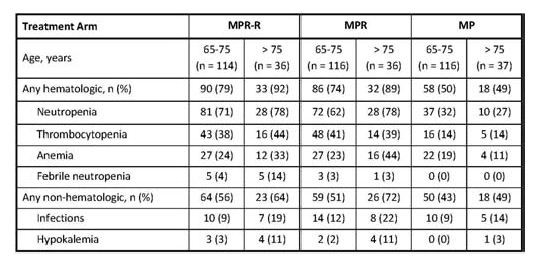
Table 1. Grade 3-4 hematologic and non-hematologic adverse events occurring in ≥ 10% of patients.
Results. A total of 152, 153, and 154 patients were randomized to MPR-R, MPR, and MP, respectively. Grade 3-4 non-hematologic AEs occurring in ≥10% are listed (Table 1). During induction in the MPR-R, MPR, or MP arms, G-CSF was used in 100 (67%), 87 (57%), and 46 (30%) of patients. Only 1%, 4%, and 1%, respectively, discontinued any drug due to neutropenia. Regarding thrombocytopenia, no bleeding events were reported. Platelet transfusions were required by 51 (34%), 41 (27%), and 25 (16%) of MPR-R, MPR, and MP patients, respectively. Discontinuation of any drug for thrombocytopenia was infrequent: 3%, 5%, and 0%. With thromboprophylaxis, grade 3-4 deep-vein thrombosis (DVT) occurred in 3% (lenalidomide-treated) patients and 1% (MP) during induction. Discontinuation from induction due to AEs occurred in 16% (MPR-R), 14% (MPR), and 5% (MP) of patients. During lenalidomide maintenance, newly occurring or worsening grade 3-4 AEs were infrequent. Grade 4 neutropenia and thrombocytopenia were reported in 2/88 (2%) and 5/96 (6%), respectively. There were no reports of grade 3-4 febrile neutropenia or bleeding events. G-CSF was administered to 27 (31%) patients; 9 (10%) patients received platelet transfusions. During maintenance, DVT was reported in 2 (2%) MPR-R and 1 (1%) MPR patients. Only 8% discontinued lenalidomide maintenance due to AEs. For induction and maintenance, discontinuation of any drug due to neutropenia was infrequent (2%, 4%, and 1%, for MPR-R, MPR, and MP, respectively). Similarly, only 3%, 5%, and 0% of patients discontinued any drug due to thrombocytopenia. Twelve (MPR-R), 10 (MPR), and 4 (MP) invasive second primary malignancies were reported, corresponding to low incidence rates per 100 patient-years of 3.04, 2.57, and 0.98, respectively. Conclusions. MPR induction AEs were manageable with dose reductions, GCSF, and platelet transfusions, allowing the majority of patients aged 65-75 years to proceed to maintenance phase. Lenalidomide maintenance was generally well-tolerated in these patients with little evidence of cumulative toxicities, permitting continuous long-term therapy. In all patients, MPR-R treatment significantly extended median PFS vs. fixed-dose MP and MPR (P<.001 for both comparisons).
Haematologica, 2012; 97(s1): 120
Datum přednesení příspěvku: 14. 6. 2012