Konference: 2015 57th ASH Annual Meeting - účast ČR
Kategorie: Mnohočetný myelom
Téma: 731. Clinical Autologous Transplantation: Results: Poster
Číslo abstraktu: 1974
Autoři: M.D. Chiara Cerrato; Francesca Gay; MD Maria Teresa Petrucci; MD Pellegrino Musto; MD Gianluca Gaidano, PhD; M.D. Massimo Offidani; Tommasina Guglielmelli; Marco Salvini; Francesca Patriarca; Elena Ponticelli; Gianpietro Semenzato; M.D. Francesco Di Raimondo; Roberto Mina; MD Nicola Cascavilla; M.D. Dina Ben-Yehuda; Daniela Oddolo, Ph.D.; M.D. Paolo Corradini; Lucio Catalano; Dr. Paolo Di Bartolomeo; prof. MUDr. Roman Hájek, CSc.; MD Andrew Spencer; MD Mario Boccadoro; MD Antonio P. Palumbo
Methods Data from newly diagnosed MM patients enrolled in 4 phase III trials were analysed. Two trials included ASCT-eligible patients: RV-MM-209 [melphalan-prednisone-lenalidomide (MPR) vs melphalan 200 mg/m2 (Mel200), followed by lenalidomide maintenance vs no maintenance), RV-MM-EMN-441 (cyclophosphamide-lenalidomide-dexamethasone vs Mel200, followed by lenalidomide vs lenalidomide-prednisone maintenance). Two studies enrolled elderly, ASCT-ineligible patients: GIMEMA-MM0305 (bortezomib-melphalan-prednisone-thalidomide followed by bortezomib-thalidomide vs bortezomib-melphalan-prednisone) and EMN01 (MPR vscyclophosphamide-prednisone-lenalidomide vs lenalidomide-dexamethasone, followed by lenalidomide vslenalidomide-prednisone maintenance). The primary endpoint of the study was to evaluate the impact of maintenance on PFS and OS in patients who achieved CR. Univariate analyses of OS and PFS were performed. Response was considered as a time-dependent variable with a landmark point at 12 months. Lastly, a multivariate analysis was performed to evaluate the impact of maintenance and ASCT as independent variables.
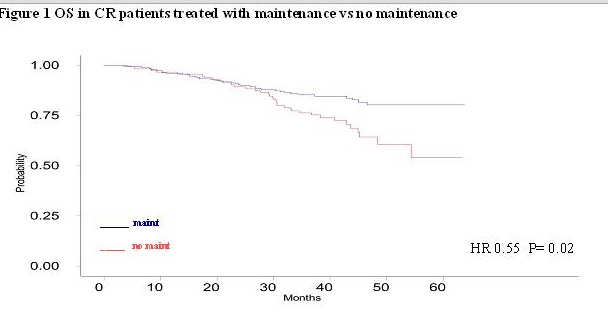
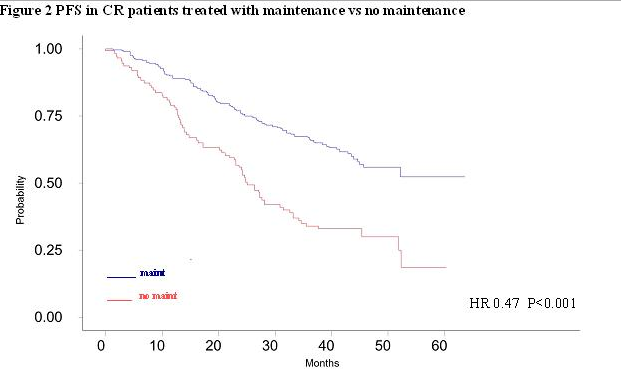
Results A total of 1964 patients were retrospectively analysed. Of 1503 patients who received maintenance therapy, 254 achieved a CR and 931 a very good partial response (VGPR) or partial response (PR). After a median follow-up of 41 months, a significant 5-year OS (80% vs 54%; HR 0.55, p=0.02; Figure 1) and 5-year PFS (52% vs 19%; HR 0.47, p<0.001; Figure 2) advantage was reported among CR patients who received maintenance in comparison with no maintenance.
The same analysis was conducted in patients achieving a suboptimal response (VGPR or PR): the 5-year PFS advantage was confirmed in patients who received maintenance vs patients who did not (30% vs 13% HR 0.65, p<0.001); the 5-year OS was 68% vs 38% in patients who received maintenance vs no maintenance respectively (HR 0.8, p=0.2).
A subgroup analysis was conducted in CR patients according to the treatment received [ASCT vs conventional chemotherapy (CC)]; the PFS benefit among patients treated with maintenance was confirmed across both the subgroups (ASCT group: HR 0.45, p=0.02; CC group: HR 0.45 P<0.001).
In multivariate analysis, maintenance therapy and treatment with ASCT confirmed the favourable impact on PFS and OS in patients achieving CR.
Conclusion In CR patients, maintenance therapy significantly prolongs PFS and OS. In order to optimize treatment efficacy and to prolong survival in patients with a sensitive disease, the intensification with maintenance is strongly recommended.
Disclosures: Off Label Use: Use off-label of drugs for the dose and/or schedule and/or association. Gay: Sanofi:Membership on an entity’s Board of Directors or advisory committees ; Janssen-Cilag: Honoraria ; Celgene:Honoraria , Membership on an entity’s Board of Directors or advisory committees . Gaidano: Novartis: Honoraria , Other: Advisory boards ; Celgene: Research Funding ; Karyopharm: Honoraria , Other: Advisory boards ; Roche:Honoraria , Other: Advisory boards ; Morphosys: Honoraria , Other: Advisory boards ; GlaxoSmithKline: Honoraria , Other: Advisory boards ; Amgen: Honoraria , Other: Advisory boards ; Janssen: Honoraria , Other: Advisory boards . Offidani: Janssen-Cilag, Celgene, Sanofi, Amgen, Mundipharma: Honoraria . Patriarca: Janssen-Cilag, Celgene, Merck Sharp & Dohme: Honoraria . Di Raimondo: Janssen-Cilag, Celgene: Honoraria . Hájek: Janssen-Cilag: Honoraria ; Celgene, Merck Sharp & Dohme: Consultancy , Honoraria . Boccadoro: Sanofi: Consultancy , Membership on an entity’s Board of Directors or advisory committees ; Celgene: Consultancy , Membership on an entity’s Board of Directors or advisory committees ; Onyx Pharmaceuticals: Consultancy , Membership on an entity’s Board of Directors or advisory committees ; Janssen-Cilag: Consultancy , Membership on an entity’s Board of Directors or advisory committees . Palumbo: Novartis, Sanofi Aventis: Honoraria ; Celgene, Millennium Pharmaceuticals, Amgen, Bristol-Myers Squibb, Genmab, Janssen-Cilag, Onyx Pharmaceuticals: Consultancy , Honoraria .
Datum přednesení příspěvku: 5. 12. 2015