Konference: 2013 18th Congress of the European Hematology Association - účast ČR
Kategorie: Mnohočetný myelom
Téma: Multiple myeloma - Translational and clinical studies
Číslo abstraktu: P221
Autoři: Francesca Gay; MD Sara Bringhen; M.D. Massimo Offidani; Prof. MD Anna Marina Liberati; Claudia Cellini; MD Valeria Magarotto; Giulia Benevolo; Gabriele Aitoro; Francesca Patriarca; Paola Omede; Concetta Conticello; MD Vittorio Montefusco; M.D. Davide Rossi; Carmela Palladino; prof. MUDr. Luděk Pour, Ph.D.; Alessandro Allegra; Giuseppe Pietrantuono; M.D. Antonietta Pia Falcone; Alberto Rocci; Renato Zambello; Antonio Ledda; Silvia Gentili; MD Pellegrino Musto; MD Mario Boccadoro; prof. MUDr. Roman Hájek, CSc.; MD Antonio P. Palumbo
Background:
Lenalidomide plus low-dose dexamethasone (Rd) and melphalan- prednisone-lenalidomide (MPR) followed by lenalidomide maintenance showed to be effective and safe in elderly newly diagnosed multiple myeloma(MM) patients (pts). Cyclophosphamide represents a valid alkylant alternative in combination with steroids and novel agents. No formal comparison between these combinations has been performed until now.
Aims:
To assess the efficacy and safety of the lenalidomide plus low dose dexamethasone (Rd) vs Melphalan-Prednisone-Lenalidomide (MPR) and Cyclophosphamide-Prednisone-Lenalidomide (CPR) in a community-based setting of MM pts ≥65 years old or not eligible to autologous stem cell transplantation.
Methods:
Pts with symptomatic MM were randomized (1:1:1) to receive 9 28- day cycles of Rd, MPR or CPR. Upfront dose reductions of dexamethasone, melphalan and cyclophosphamide were performed, according to pt age (Rd: lenalidomide 25 mg/day for 21 days; dexamethasone 40 mg on days1, 8, 15 and 22 in pts 65-75 years old and 20 mg in those >75 years; MPR: lenalidomide 10 mg/day for 21 days; melphalan orally 0.18 mg/Kg for 4 days in pts 65-75 years old and 0.13 mg/Kg in >75 years pts; prednisone 1.5 mg/Kg for 4 days; CPR: lenalidomide 25 mg/day for 21 days; cyclophosphamide orally 50 mg/day for 21 days in pts 65-75 years old and 50 mg every other day (eod) in >75 years pts; prednisone 25 mg eod). After induction, pts were randomized to receive maintenance with lenalidomide (10 mg/day on day 1-21 every 28) alone or in combination with prednisone (25 mg eod), until disease progression. The primary endpoint was progression-free survival (PFS).
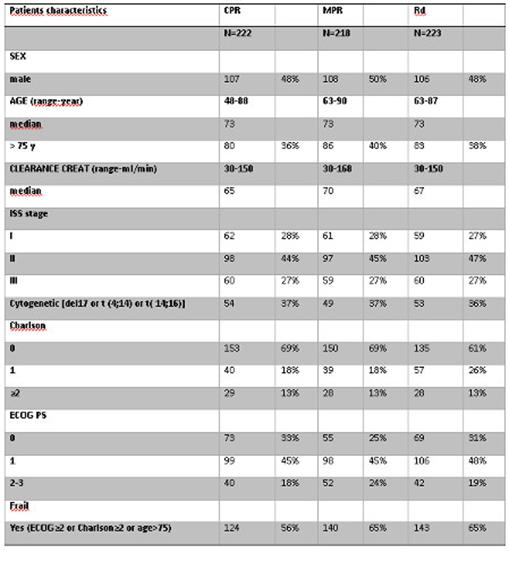
Results:
Between October 2009 and October 2012, 663 pts were enrolled (Rd:222, MPR:218; CPR: 223). Patient characteristics were well balanced in the three groups. Median age was 73 years in each arm; 37%, 40% and 36% of pts respectively in Rd, MPR and CPR arms were >75 years. Frail pts were 65% in the Rd arm, 65% in the MPR arm and 56% in CPR arm. (Table). At data cut-off all pts had completed the 9 induction cycles. Median follow-up was 19 months. Partial response (PR) rate was similar in the 3 arms: 74%, 74% and 75% respectively in Rd, MPR and CPR group, including 35% very good partial response in Rd, 29% in MPR and 26% in CPR. A trend towards a higher complete response (CR) rate was noticed in the MPR group (12%), similar CR rate was reported in Rd (5%) and CPR (7%). At least 1 grade ≥3 hematological adverse event (AE) was reported in 28% Rd pts, 62% MPR pts and 29% CPR pts. The main hematological AE was neutropenia (Rd: 24%; MPR: 59%; CPR: 26%). At least 1 grade ≥3 non-hematological AE was observed in 25% of Rd pts, 29% of MPR pts and 22% of CPR pts. The most common grade ≥3 non-hematological AEs were infections (Rd: 6%, MPR: 9%, CPR:4%) and dermatological toxicities (Rd: 4%, MPR: 4%, CPR: 7%). Treatment discontinuations for toxicity were 7% in Rd, 12% in MPR and 12% in CPR. The main reason for treatment discontinuation was non-hematological toxicity in Rd (6%) and CPR (11%). Only 1% of pts stopped treatment for hematological AEs in Rd and CPR. In the MPR arm 7% of pts stopped treatment for hematological AEs and 5% for non-hematological AEs. Rate of toxic deaths was similar in the 3 arms (4% Rd, 4% MPR and 5% CPR).
Datum přednesení příspěvku: 14. 6. 2013