Konference: 2015 20th Congress of the European Hematology Association - účast ČR
Kategorie: Mnohočetný myelom
Téma: Poster
Číslo abstraktu: P270
Autoři: MD Alessandra Larocca; MD Sara Bringhen; MD Maria Teresa Petrucci; M.D. Massimo Offidani; MD Lorenzo De Paoli; Giuseppe Pietrantuono; Luca Baldini; Tommasina Guglielmelli; MD Valeria Magarotto; Maria Cantonetti; MD Andrea Nozza; Andrea Evangelista, PhD; Stefano Spada; Prof. M.D. Nicola Giuliani; MD Mariella Grasso; M.D. Roberto Marasca; MD Vittorio Montefusco; Dott.ssa Iolanda Donatella Vincelli; MD Fortunato Morabito; Chiara (Clara) Nozzoli; Luca De Rosa; Maide Cavalli; M.D. Angelo Michele Carella; prof. MUDr. Roman Hájek, CSc.; MD Mario Boccadoro; MD Antonio P. Palumbo
Background
Early mortality in elderly multiple myeloma (MM) patients is
usually attributed to combined effects of active disease and
co-morbid factors. Before the introduction of novel agents, toxic
deaths within 60 days from start of conventional treatment occurred
in 10% of patients (Augustson BM. J Clin Oncol 2005, 36:9219),
mainly due to infection and renal failure. The use of novel agents
has considerably improved MM outcome at the expense of newer
toxicity.
Aims
The aim of this analysis is to study early deaths not related to
disease progression during treatments with lenalidomide or
bortezomib. We analyzed individual patient data from two large
multicenter randomized trials to assess the rate and the causes of
death, their predictability and whether current management
strategies have reduced their frequency.
Methods
A total of 1,173 newly diagnosed MM patients ineligible for
autologous transplantation due to age or co-morbidities
enrolled in the Gruppo Italiano Malattie EMatologiche
dell’Adulto (GIMEMA) and European Myeloma Network (EMN) trials from
May 2006 to September 2012, were studied. Patients in the GIMEMA
MM-03-05 trial (N=511) received bortezomib-containing regimens
(Palumbo A. J Clin Oncol 2014, 32:634) and those in the EMN01 trial
(N=662) lenalidomide-containing regimens (Magarotto V. Blood 2014,
abs ASH).
Results
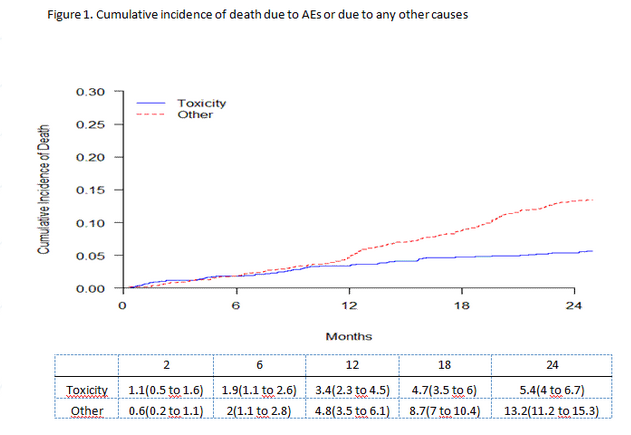
A total of 1146 patients could be evaluated for this analysis.
Within 24 months from start of therapy, 207/1146 patients (18%)
died for any causes, 61/1146 (5%) died due to adverse events. Toxic
deaths within 60 days occurred in 12 patients (1%) with a linear
increase over time of 1% every 6 months (Figure 1). There was no
difference in the incidence of toxic deaths between patients
receiving bortezomib-containing regimens (31 pts, 6%) and those
receiving lenalidomide-containing regimens (30 pts, 5%, p=0.32).
The incidence of toxic deaths was significantly higher in patients
older than 80 years (11/107 [10%], p=0.005). Twenty-nine percent of
deaths were attributable to cardiac complications (18 pts), 18% to
infections (17 pts) and 15% to vascular complications (9 pts). By
comparing the cause of toxic deaths between the 2 different
treatment regimes, there was no significant difference in the
proportions of cardiac events, infections, vascular events or other
causes. In a multivariate analysis, age (HR 1.09 per 1 year
increase, p=0.002) and ISS score (HR 3.81, p=0.01 ISS 2 vs ISS 1;
HR 5.69, p=0.002 ISS 3 vs ISS 1) did increase the risk of death but
poor performance status did not (HR 1.25, p=0.59). Greater tumor
burden and activity (ISS) increased the risk of death because such
deaths occurred before the maximal beneficial effect of therapy in
reducing tumor load: 92% of patients dying from toxicity within 2
months of start of therapy had achieved a suboptimal response (8
not available, 3 SD, 1 PR, ORR 8%).
Summary
Novel, more effective and more rapid therapies have reduced the
risk of toxic deaths as compared to conventional treatments.
Nevertheless one-third of early deaths occurred primarily due to
cumulative specific drug-related toxicities. Improvement in
supportive therapy together with prevention and prompt
recognition/treatment of complications are urgently needed to
reduce the risk of toxic deaths. The 2-fold higher risk of toxic
mortality in octogenarians indicates the need for a careful
assessment of frail patients who may benefit from a gentle or even
palliative approach.
Keyword(s): Elderly, Imids, Mortality, Proteasome
inhibitor
Datum přednesení příspěvku: 12. 6. 2015